


The health component of the Budget focused on NDIS cost-cuts. Not much else changed, leaving fundamental flaws in the health industry unresolved. Claudia Weisenberger reports.
In 2023/24, major health insurers posted $2.11B in pre-tax profits according to APRA. The share of premium dollars reaching hospitals fell from 90% (pre-COVID) to about 84% by 2022/23, with the latest data (December 2025) showing modest improvement to 86.3%, still short of the 90% benchmark.
Public elective surgery waiting lists grew 41.6%.
The subsidies were $6.5B in 2022/23, increasing to $6.9B in 2023/24 and to $7.9B this financial year, a 23% increase from the 2012-13 baseline.
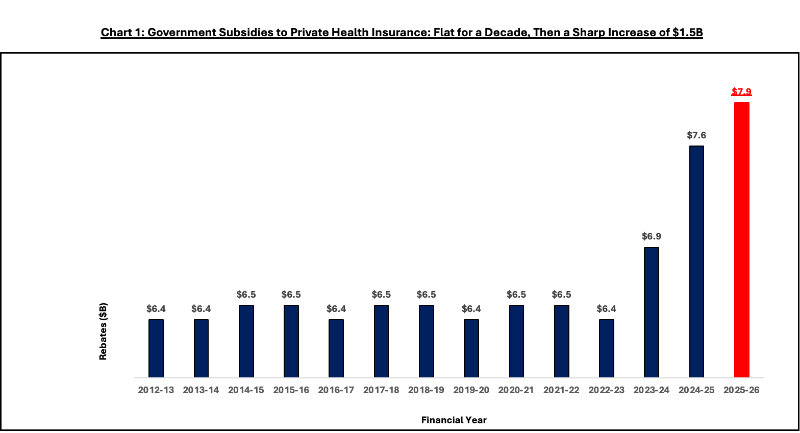
Source: Australian Government Budget Papers 2012-13 through 2025-26.
Meanwhile, insurer profits remain strong while the hospital funding share stay below pre-COVID levels, and public waiting lists continue to grow, as hospitals close.
Health insurance industry to protest rebate changes as hospitals close
If escalating subsidies are not preventing hospital closures, restoring hospital funding ratios, or relieving public waiting list pressure, what policy goal justifies the expenditure?
Opportunity cost
Every rebate dollar is a dollar not enabling Australians to build health savings, or flowing to public hospitals serving all Australians, including the chronically ill, low-income, and disrupted-employment cohorts that the Private Health Association (PHA) invokes when defending community rating.
The $7.9B flows to an industry posting $2B+ in profits while reducing hospital funding shares. Public hospitals saw waiting lists grow by 433,000 patients. The equity question: should $7.9B continue subsidising industry profits, or enable individual health savings while strengthening public capacity?
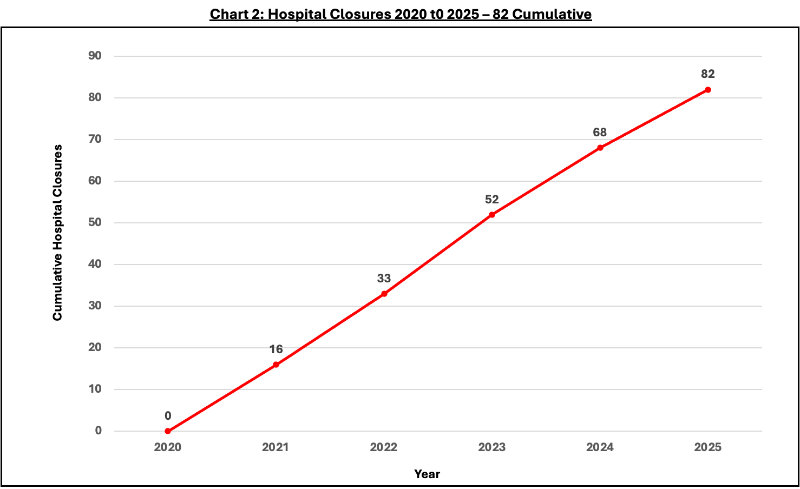
Source: Australian Private Hospitals Association.
Geographic distribution matters. A metropolitan day surgery does not replace a regional full-service hospital. Lost service categories, including private maternity care, which is projected to be extinct by decade’s end, do not appear in facility counts.
The PHA is dismissive of hospital underfunding claims, but the numbers tell a different story.
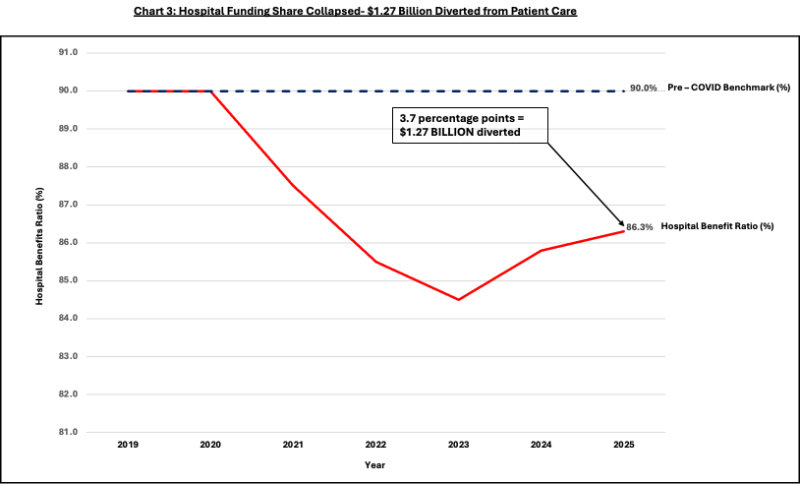
Source: APRA Quarterly Private Health Insurance Statistics.
Government evidence
A 2023 Finity report commissioned by the Health Department found cutting over-65 rebates would save $482 million in rebate costs but shift $547 million to the public system, a net loss.
Health Minister Mark Butler scrapped these rebates anyway, calling them ‘unfair’—despite his own department’s advice. The contradiction reveals the core problem: not whether subsidies are necessary, but where the money goes.
When $7.9B generates $2B in profits while hospital shares fall from 90% to 86.3%, the question is allocation.
A reasonable next step would be to introduce independent disclosure. An open reconciliation of insurer-to-hospital funding flows, audited and published, mandatory publication of funding flows, premium-to-benefit ratios by tier and product, and data underlying disputed claims would resolve these questions definitively.
What’s ‘good’ value?
Does $7.9B in annual subsidies deliver value commensurate with cost?
Record profits, falling hospital shares, 82 closures, and 41.6% waiting list growth sit alongside a subsidy that grew $1.5B from its 2012-13 baseline. Every dollar subsidising profits is a dollar not flowing to individual health savings Australians own, or to public capacity serving the majority.
Singapore demonstrates that health savings accounts, catastrophic insurance, and robust safety nets deliver superior outcomes at lower cost.[7] Australia could redirect a portion of the $7.9B toward individual accounts while strengthening public capacity.
The question is not whether to support healthcare. It is whether the current allocation serves Australians well. The numbers suggest it does not.
Private health care. Why community ratings are failing the young

Claudia Weisenberger is a management consultant with deep experience in pharmaceuticals, hospital transformations, and strategic due diligence across four continents. She combines sharp analysis with hands-on execution.