


The NDIS was designed for people who need support for the rest of their lives, but who they are has never been properly defined. Claudia Weisenberger proposes a way forward.
A 26-year-old Australian woman has never spoken a word. She cannot be left alone for an hour. Her parents lock the fridge; otherwise, she raids it constantly for the unhealthiest foods she can find. She requires around-the-clock care, every day, with no end in sight.
A 65-year-old man who has been quadriplegic since a car accident at 21. Four decades of navigating disability support, understanding from the inside what serious permanent disability actually requires.
Both are exactly who the NDIS was built for. And yet the scheme they rely on also supports one in six boys in a Grade 2 classroom, most with an autism or developmental delay diagnosis. In some parts of the country, it is one in four. These are not the same needs.
And the scheme cannot tell the difference.
What these two examples share is not a diagnosis. It is permanent impairment — what they cannot do, regardless of any intervention, for the rest of their lives. The NDIS was built for that.
What NDIS was built for
The NDIS Act is precise: a permanent, likely lifelong disability attributable to an impairment that substantially reduces functional capacity to undertake a range of activities, and the capacity for social or economic participation.
Section 24 of the Act sets a high bar: substantially reduced functional capacity, permanently. It never says how that must be proven. Into that silence. The NDIA built List A, an internal administrative guideline, not a legislative instrument, listing diagnoses that qualify automatically. It is a shortcut that lets a diagnosis alone stand in for proof, and because it sits in agency policy rather than the Act itself, it is also a shortcut the NDIA could tighten without parliament’s involvement.
The Act asked the right question. It just never demanded an answer.
List A is precise about which diagnoses automatically qualify: autism at Level 2 or 3, cerebral palsy, and a defined set of other conditions. The threshold exists on paper. But Level 1 autism, the mild end of the same spectrum, can still qualify through clinician-reported evidence of functional impact, with no independent assessment required to verify that claim.
A child who finds group work difficult. A teenager who struggles to make friends. An adult who gets anxious at a party. Their diagnosis may be Level 1. Their clinician’s report says their functional capacity is substantially reduced. Nobody checks.
Diagnosis filled the gap, and it became the gateway. But the gateway was never properly guarded.
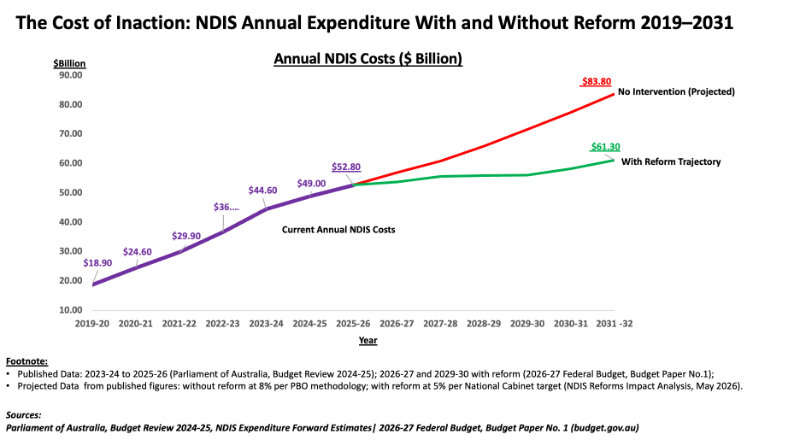
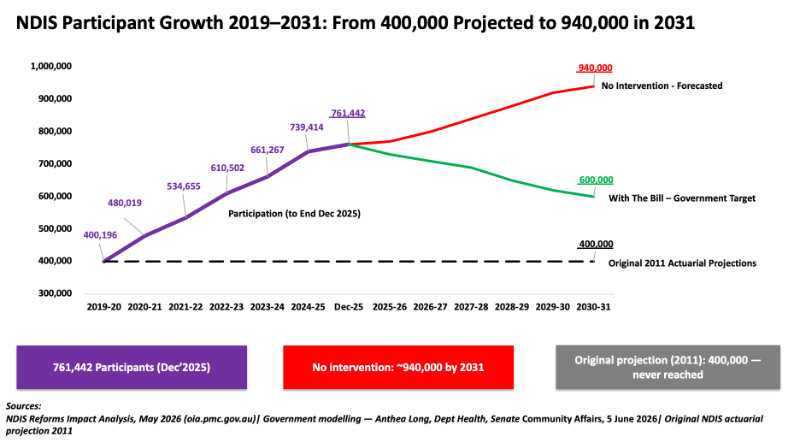
The scheme’s designers projected 400,000 participants at a cost of $13.6B annually. In December 2025, there were 761,442 participants.
In 2024-25, the NDIS spent $49B, more than Medicare, which covered 27.5 million Australians for $32.8 billion (Services Australia Annual Report 2024-25).
Where the money goes
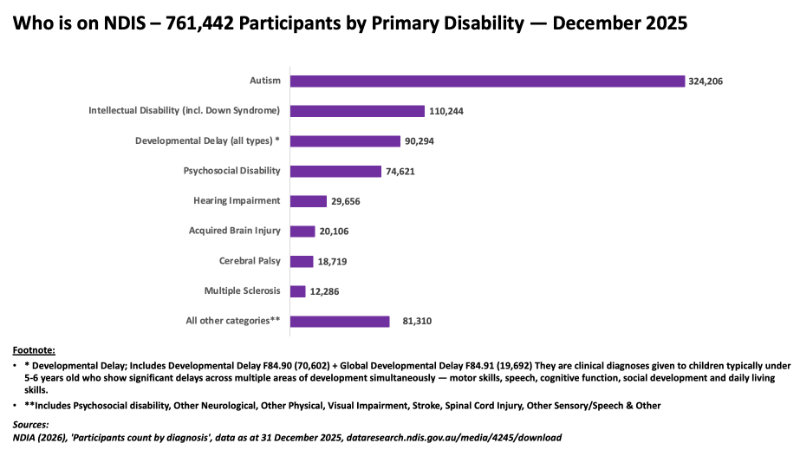
Autism, 324,206 participants, 43% of the scheme, up 51% in two and a half years. The spectrum spans from those who cannot speak to those who live, study and work independently. The diagnosis is identical. The impairment is not. That distinction is the one List A was never designed to make.
Developmental delay, 90,294 participants, coded by the NDIA as ‘not to be used over 6 years of age’: a temporary placeholder, not a permanent condition.
Psychosocial disability, approximately 74,621 participants, 10% of the scheme, conditions that respond to medical treatment are health needs, not disability support needs.
Permanent, treatment-resistant conditions belong in the NDIS. The distinction is whether treatment exists. Together these three categories account for approximately two-thirds of the scheme. The government’s own Impact Analysis (May 2026) names the mechanism: ‘an over-reliance on access lists based on diagnosis rather than impairment.’
A diagnosis is not an impairment.
The NDIA’s own commissioned evidence review found ‘almost no evidence about the effects of intervention practices on quality-of-life outcomes.’ 78% of all children under 8 in the scheme carry one of these diagnoses. That is the scale of the drift from the scheme’s founding purpose.
Every dollar allocated to a plan that does not reflect genuine permanent disability is a dollar unavailable to the people this scheme was built for.
A 57% psychology shortfall and a 77-day average wait for a psychiatrist is not a mental health system. It is a waiting room for the NDIS.
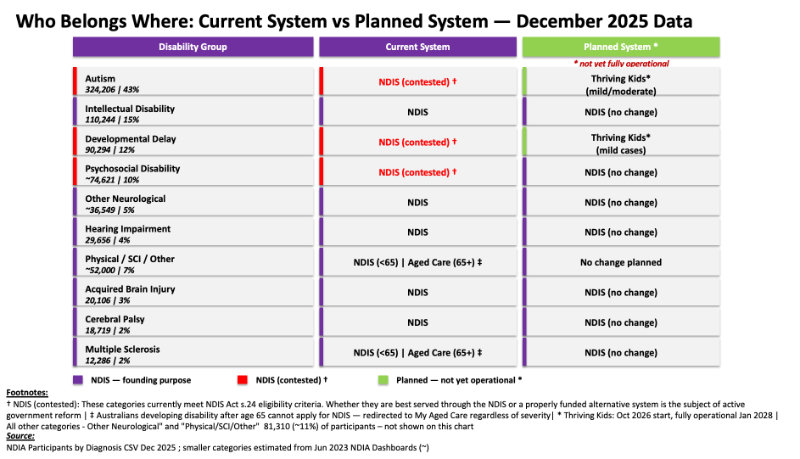
This is not an argument against support, but an argument about which system provides it. Thriving Kids, commencing October 2026, is designed for these children. It should be fully operational before any gate closes.
The fix
The tools already exist: occupational therapists use validated functional assessments, including the WHODAS 2.0, the Katz ADL scale, the COPM, and the Care & Need Scale (CANS), used to assess precisely what a person can and cannot do independently.
What has never existed is the requirement to apply them before granting access. Currently, under List A, a diagnosis alone is sufficient. That is the gap.
An independent assessment would close that gap.
The NDIS was built for disability support needs. It was not built for health needs, however serious or chronic. That line has not been drawn clearly.
Lessons from other countries
In 1990, the Netherlands spent 4.7% of GDP on disability insurance — more than three times the OECD average. The Dutch didn’t cut, they redefined the question. Function, not diagnosis. Rehabilitation before support. New applications fell 40%.
The lesson is one of design, not spending levels.
New Zealand drew one line Australia never drew: where a condition requires ongoing health professional supervision, that person has a health need, not a disability support need. Renal dialysis goes to the health system. Community services before specialist disability services. The NDIS has neither.
Both countries ask the question Australia has avoided: not ‘what is your diagnosis?’ but ‘what can you do independently, and is that permanent?’
A review across Norway, Sweden, the UK and Canada found that tightening disability eligibility without building adequate alternatives shifted people from disability schemes to other benefit systems. The harm did not disappear. It moved.
What’s the Government proposing?
The NDIS Amendment Bill proposes removing 350,000 participants by 2031 from a scheme the NDIA cannot properly describe or measure, without requiring the functional assessments that already exist, and
before the alternatives are in place.
The government legislated changes in October 2024, redefining what can be funded. The question of who belongs does not take legal effect until January 2028. The Netherlands built first. New Zealand built first. Australia cuts first.
The people who will bear the cost of getting this wrong are the 26-year-old who has never spoken and the man who has been quadriplegic for 44 years. The question is not whether the NDIS is too big. It is whether Australia is finally willing to define what it was built for, and build everything else first.

Claudia Weisenberger is a management consultant with deep experience in pharmaceuticals, hospital transformations, and strategic due diligence across four continents. She combines sharp analysis with hands-on execution.