

The NDIS was meant to create competition to keep disability service prices low. Instead, most service providers charge the maximum allowed. Claudia Weisenberger reports.
The majority of NDIS providers who reported in the NDIA’s own Financial Benchmarking Survey conceded they always set prices at the maximum allowed rate. It is a self-reported figure from 2020-21, and it has not been updated since. But it is corroborated by something more recent and more robust: transaction data.
The independent NDIS Review, published in 2023, analysed actual billing records across the scheme. It found that 83% of all price-capped transactions occur at or close to the ceiling. The review was blunt in its assessment. Price caps, it found, are not functioning as price ceilings.
They are functioning as price anchors.
Two independent data sources. Five years apart. The same finding.
Market not working
When the NDIS was designed, its pricing framework rested on a specific theory. Published price ceilings would prevent exploitation. But below those ceilings, providers would compete — on quality, on convenience, on service — and participants with genuine choice and control would benefit from market forces that kept prices efficient.
In practice, the competitive market has not materialised. Participants with disability are not, in most cases, in a position to shop around and negotiate. Their support needs are specific, their options are often limited by geography or disability type, and they bear no direct financial cost from paying the ceiling rate. The result is a market in which the published maximum has become — in almost every transaction — the actual price.
A price ceiling is only useful if providers have an incentive to charge below it. In the NDIS, 83% of providers never do.
The support workers gap
The support worker category illustrates the pricing structure most clearly. The 2025-26 NDIS price limit for standard weekday disability support work is $70.23 per hour. The worker doing the job earns $34.58 per hour under the SCHADS Award, the minimum wage framework governing the sector. The $35.65 difference pays for superannuation, insurance, administration, compliance and margin.
These are legitimate costs in any service industry. The question is not whether they exist — it is whether a market in which 83% of providers charge the maximum has any mechanism to reduce them.
The 83% figure does not indicate widespread dishonesty among providers. It indicates a pricing system so poorly designed that charging the maximum is
the rational response to the incentives it creates.
The therapy rate cut
In its 2025-26 Annual Pricing Review, the NDIA did something it had never done before: it cut the physiotherapy rate. The rate fell from $193.99 to $183.99 per hour — a 5.2% reduction — after its own benchmarking analysis found the existing rate was above the average fully loaded cost of most therapy professionals.
The NDIA drew on more than ten million transactions and compared NDIS rates against Medicare and private health insurance data for the first time.
What it found went well beyond physiotherapy. The 2024/25 Annual Pricing Review found that many NDIS therapy pricing limits were out of step with broader market rates — in some cases exceeding them by up to 68%. This was the NDIA’s own benchmarking conclusion, drawn from its own data. Occupational therapy, speech pathology, behaviour support and support coordination rates were not reduced.
NDIS vs Medicare pricing
Autism and developmental delay account for 45% of all NDIS participants — the single biggest driver of therapy demand in the scheme. Physiotherapy alone represents approximately 1% of total NDIS annual expenditure. Total therapy spending across all disciplines is calculated to be approximately $5B.
The table below shows where NDIS rates sit relative to what Medicare covers. The contrast is stark — and the core structural failure is not simply the level of rates. It is that no competitive mechanism exists to test whether those rates are fair.
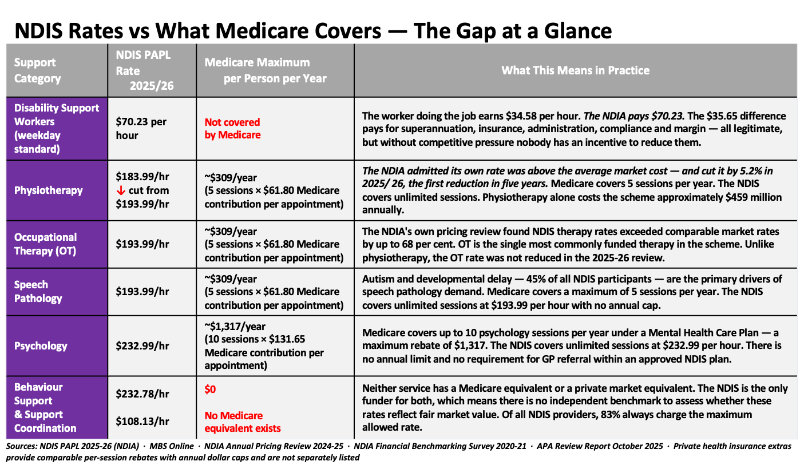
Note: Medicare rebates under the GPCCMP (GP Chronic Condition Management Plan) require a GP referral and a diagnosed chronic condition. The 5 sessions are shared across all allied health disciplines — not 5 sessions per discipline. Private health insurance extras are not included.
The solution
A further distinction: Medicare enables co-payments — the gap between the rebate and the provider’s fee is paid by the patient out of pocket, creating at least some price signal. The NDIS does not. Participants pay nothing directly, which
removes the incentive to question whether the price is fair.
The NDIS Review recommended moving towards independent pricing, yet the NDIA has historically set its own prices, assessed whether those prices are fair, and reported on the outcomes, all without independent oversight. The Productivity Commission warned in 2017 this creates an incentive to use pricing as a budget lever rather than a market development tool.
In every other major government-funded healthcare sector in Australia, at least one of those three functions is performed independently. In the NDIS, none of them are.
A more effective solution than a price ceiling — which has become a price floor — is a published reference price with an automatic flagging mechanism. Any claim above the reference price triggers a review before payment is released. Providers with genuine cost justifications can still be paid. Those without one cannot.
The burden shifts from the NDIA attempting to detect anomalies after payment has been made to providers justifying exceptions before it is made.
The question is not whether to pay providers fairly;
it is whether the current pricing mechanism is producing fair prices at all.
Disability support work is genuinely complex. But a price ceiling set above market rates, charged at the maximum by virtually every provider, in a market where participants cannot effectively negotiate, is not a competitive market.

Claudia Weisenberger is a management consultant with deep experience in pharmaceuticals, hospital transformations, and strategic due diligence across four continents. She combines sharp analysis with hands-on execution.